Charles River Analytics, developer of intelligent systems solutions, announces a follow-on contract for a system to automatically sense indicators of cognitive workload for battlefield medics. Military medical personnel may be deployed to operational environments where their success in saving lives depends on their ability to act quickly and effectively, both as individuals and in teams. Currently, trainers must infer competence by observation of behaviors and decisions alone, which does not provide insight into more unobservable factors that may provide better indicators of cognitive performance. Effective operational training must go beyond the training of individual skills to include training of interactions among team members, and how those interactions transfer to effective operations. Charles River Analytics’ system to augment training by Monitoring, Extracting, and Decoding Indicators of Cognitive Load, or MEDIC, will assist in training military medical personnel. The 30-month contract awarded by the US Army is valued close to $1 million.
Charles River is designing the MEDIC system as a multi-modal suite of unobtrusive, field-ready neurophysiological, physiological, and behavioral sensors. MEDIC automatically senses indicators of cognitive workload to augment performance observations, offering insight into factors underlying that performance.
“We have completed the initial design and testing of MEDIC on a two-person team,” said Dr. Bethany Bracken, a scientist at Charles River Analytics, and Principal Investigator on MEDIC. “We will now iteratively evaluate and validate the MEDIC system starting in a laboratory environment, at a medical school simulation center, and finally at a full-scale Army medic simulation environment.”
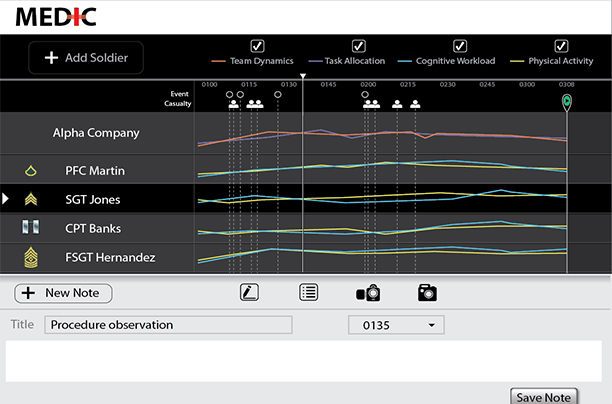
This figure displays the MEDIC user interface. The trainer can review the details of training performance in this after action review screen.
The MEDIC system is poised to have far reaching benefits, improving training outcomes or a number of emergency management training groups, including the Federal Emergency Management Agency (FEMA), state and local governments, as well as in applications for training emergency medical personnel and first responders.
This work is supported by the US Army Medical Research and Materiel Command under Contract No: W81XWH-14-C-0018. The views, opinions and/or findings contained in this report are those of the author(s) and should not be construed as an official Department of the Army position, policy or decision unless so designated by other documentation.
In the conduct of research where humans are the subjects, the investigator(s) adhered to the policies regarding the protection of human subjects as prescribed by Code of Federal Regulations (CFR) Title 45, Volume 1, Part 46; Title 32, Chapter 1, Part 219; and Title 21, Chapter 1, Part 50 (Protection of Human Subjects).